TOTAL HIP REPLACEMENT SURGERY
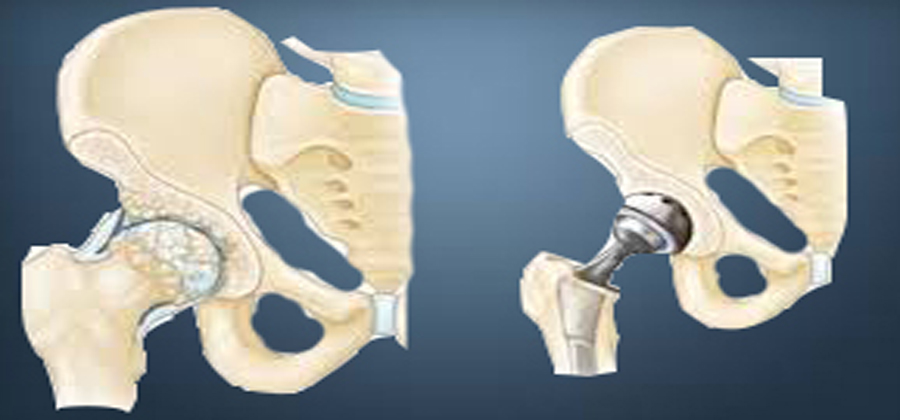
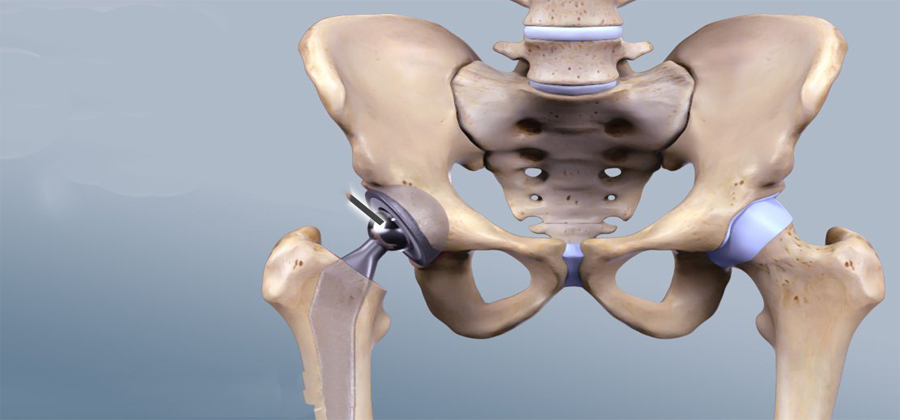
A total hip replacement is a surgical procedure whereby the diseased cartilage and bone of the hip joint is surgically replaced with artificial materials. The normal hip joint is a ball and socket joint. The socket is a "cup-shaped" component of the pelvis called the acetabulum. The ball is the head of the thighbone (femur). Total hip joint replacement involves surgical removal of the diseased ball and socket and replacing them with a metal (or ceramic) ball and stem inserted into the femur bone and an artificial plastic (or ceramic) cup socket. The metallic artificial ball and stem are referred to as the "femoral prosthesis" and the plastic cup socket is the "acetabular prosthesis." Upon inserting the prosthesis into the central core of the femur, it is fixed with a bony cement called methylmethacrylate. Alternatively, a "cementless" prosthesis is used that has microscopic pores which allow bony ingrowth from the normal femur into the prosthesis stem. This "cementless" hip is felt to have a longer duration and is considered especially for younger patients. Total hip replacement is also referred to as total hip arthroplasty.
Complications:
The risks of total hip replacement include blood clots in the lower extremities that can travel to the lungs (pulmonary embolism). Severe cases of pulmonary embolism are rare but can cause respiratory failure and death. Other problems include difficulty with urination, local skin or joint infection, fracture of the bone during and after surgery, scarring, limitation of motion of the hip, dislocation of the hip replacement, and loosening of the prosthesis that eventually leads to prosthesis failure. Because total hip joint replacement requires anesthesia, the usual risks of anesthesia apply and include heart arrhythmias, stroke, liver toxicity, and pneumonia.
Procedure:
The preoperative evaluation generally includes a review of all medications being taken by the patient. Anti-inflammatory medications, including aspirin, are often discontinued one week prior to surgery because of the effect of these medications on platelet function and blood clotting. Other preoperative evaluations include complete blood counts, electrolytes (potassium, sodium, chloride), blood tests for kidney and liver functions, urinalysis, chest X-ray, EKG, and a physical examination. Your physician will determine which of these tests are required, based on your age and medical conditions. Any indications of infection, severe heart or lung disease, or active metabolic disturbances such as uncontrolled diabetes may postpone or defer total hip joint surgery.
If the condition of the hip allows it, some doctors will recommend a preoperative exercise program to build muscle and increase flexibility. This can help with recovery.
Total hip joint replacement can involve blood loss. Patients planning to undergo total hip replacement often will donate their own (autologous) blood to be stored for transfusion during the surgery. Should blood transfusion be required, the patient will have the advantage of having his or her own blood available, thus minimizing the risks related to blood transfusions.
Recovery:
A total hip joint replacement takes approximately two to four hours of surgical time. The preparation prior to surgery may take up additional time. After surgery, the patient is taken to a recovery room for immediate observation that generally lasts between one to four hours. The lower extremities will be closely observed for both adequate sensation and circulation. If unusual symptoms of numbness or tingling are noted by the patient, recovery room nurses are available and should be notified by the patient. Upon stabilization, the patient is transferred to a hospital room. Pain-control medications are commonly given through a patient-controlled-analgesia (PCA) pump whereby patients can actually administer their own dose of medications on demand. Pain medications occasionally can cause nausea and vomiting. Antinausea medications may then be given.
Patients may also experience difficulty with urination. This difficulty can be a side effect of medications given for pain. As a result, catheters are often placed into the bladder to allow normal passage of urine. Immediately after surgery, patients are encouraged to frequently perform deep breathing and coughing in order to avoid lung congestion and the collapse of tiny airways in the lungs. Patients are also given a "blow bottle," whereby active blowing against resistance maintains the opening of the breathing passages.
Rehabilitation process
After total hip joint replacement surgery, patients often start physical therapy immediately! On the first day after surgery, it is common to begin some minor physical therapy while sitting in a chair. Eventually, rehabilitation incorporates stepping, walking, and climbing. Initially, supportive devices such as a walker or crutches are used. Pain is monitored while exercise takes place. Some degree of discomfort is normal. It is often very gratifying for the patient to notice, even early on, substantial relief from the preoperative pain for which the total hip replacement was performed.
Physical therapy is extremely important in the overall outcome of any joint replacement surgery. The goals of physical therapy are to prevent contractures, improve patient education, and strengthen muscles around the hip joint through controlled exercises. Contractures that can cause limitation of joint motion result from scarring of the tissues around the joint. Contractures do not permit full range of motion and therefore impede mobility of the replaced joint. Patients are instructed not to strain the hip joint with heavy lifting or other unusual activities at home. Specific techniques of body posturing, sitting, and using an elevated toilet seat can be extremely helpful. Patients are instructed not to cross the operated lower extremity across the midline of the body (not crossing the leg over the other leg) because of the risk of dislocating the replaced joint. They are discouraged from bending at the waist and are instructed to use a pillow between the legs when lying on the non-operated side in order to prevent the operated lower extremity from crossing over the midline. Patients are given home exercise programs to strengthen the muscles around the buttock and thigh. Most patients attend outpatient physical therapy for a period of time while incorporating home exercises regularly into their daily living.